
“Refractory” celiac disease in a 4 year old girl
History at 22 months of age
Recurrent vomiting, constipation, 2 kg weight loss, iron deficiency anemia
Mother has celiac disease
CeD-Serology (tissue transglutaminase antibodies, TGA)
at pediatrician (Lab A)
- TGA-IgA = >200 RE/ml (normal <20 U/ml)
at hospital (Lab B)
- TGA-IgA = >128 U/ml (normal <7 U/ml),
- TGA-IgG 8.6 U/ml (normal <7)
Histopathology: Marsh 3c
Diagnosis: Celiac disease
Start of strict gluten free diet (GFD)
Follow up: Vomiting and anemia resolved, good weight gain, but new symptoms: abdominal pain, bloating and diarrhea
CeD-Serology at pediatrician (Lab A): 8, 9, 13 und 15 months after starting strict GFD:
TGA-IgA = >200 RE/ml (normal <20 U/ml) all 4 time points
EMA-IgA 1:1280 (15 months after start of GFD)
Age 3.5 years (20 months after starting strict GFD)
EGD & colonoscopy because of symptoms and no decline of CeD specific autoantibodies
Histopathology: Duodenum Marsh 3b, other gastric and colonic biopsies normal
Diagnosis: Refractory celiac disease Type 1
Age 4 years: Referal to Celiac Center at Dr von Hauner Children’s Hospital, University of Munich, because of »refractory CeD« and continous diarrhea while keeping strict GFD since 2.2 years
Biopsies taken 6 months ago were reassessed by pathoolgists in Munich and Marsh 3b was confirmed.
Physical examination: very active child, except little distended abdomen perfectly normal, growth since diagnosis along the 60th percentile
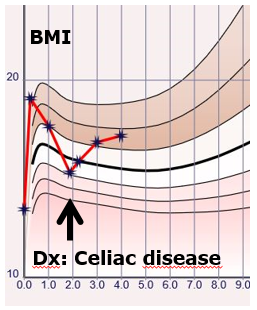
BMI: increase from the 25th to the 88th percentile for age and sex (Fig. 1)
Dietary assessment: No evidence of gluten ingestion, high intake of energy and fructose, 3 L of diluted apple juice/per day
EGD: normal duodenal villi
Histopathology : Marsh 0
CeD-Serology: TGA-IgA 30 U/ml (normal <7I
Diagnosis Celiac disease in remission, Symptoms due to overfeeding and excess of juice with fructose malabsorption.
Treatment: Energy and fructose restrictions, symptoms resolved
Take home messages:
- Refractory CeD does not exist in childhood.
- Perform titration of TGA concentrations above measuring range to judge whether TGA concentrations decline during GFD.
- Serology and histopathology may take up to 2.5 years to normalize in cases with total villous atrophy and very high TGA concentrations.
- BMI development was against the diagnosis of „malabsorption syndrome“ as obligatory sign of refractory CeD.
- Always consider other causes if „pieces of the puzzle“ do not fit in CeD. Clinical history (high juice intake) and physical examination (BMI during follow up) give the hind to solve the case.